

Abstract
Purpose
Mutations of the isocitrate dehydrogenase-1 (IDH1) and IDH2 genes are one of the most frequent alterations in acute myeloid leukemia (AML) and can be found in ~20% of patients at diagnosis. Several IDH inhibitors are currently in late stage clinical development with Enasidenib, an IDH2 inhibitor, being recently approved by the FDA. Previous analyses have reported differential impact on response to chemotherapy and outcome, depending on the IDH-mutation type, co-occurring mutations and cytogenetic abnormalities, as well as the variant allele frequency (VAF) of IDH mutations. In order to better understand its prognostic role, we analyzed newly diagnosed AML patients enrolled in prospective trials of the Study Alliance Leukemia (SAL) to investigate the impact of IDH1/2 mutations on outcome.
Patients and Methods
All AML patients consecutively enrolled into intensive AML treatment protocols of the SAL or into the SAL registry were included in this analysis. Next-generation sequencing (NGS) on an Illumina MiSeq-system was performed to detect IDH1/2 mutations using pre-treatment samples.
Overall survival (OS) and response to therapy were analyzed for all patients with intensive treatment and according to the mutational status.
Results
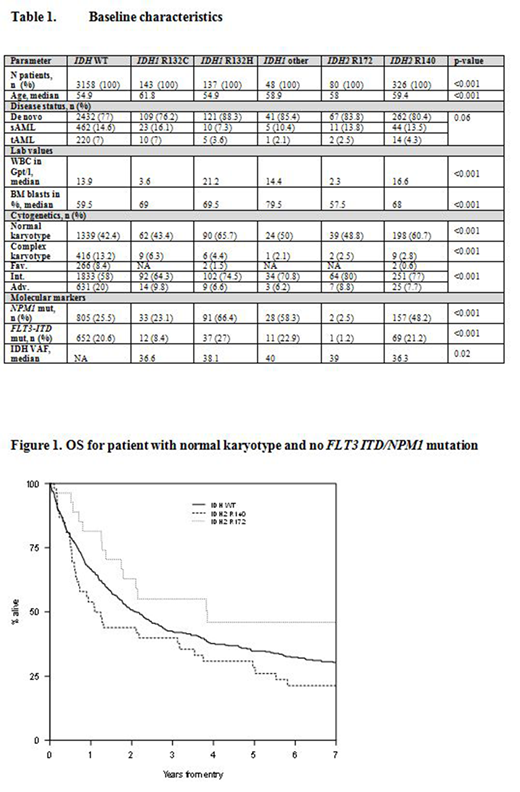
Overall, samples of 3898 patients were analyzed. The median follow-up was 91 months (95% CI 87.2 - 93.9). Patients' characteristics are shown in Tbl.1.
Three-hundred twenty-nine patients (8.4%) had IDH1 mutations and 423 (11%) had IDH2 mutations; both mutations were found in 12 pts, so the overall mutation rate in IDH1 and 2 was 19% (740/3898 patients).
Of the IDH1 variants, the most common ones were the R132C found in 143 patients (43%) and R132H in 137 patients (42%). For IDH2, 324 patients had the R140Q (77%) and 80 patients the R172K (19%) variant.
According to the two main variants of the more common IDH2 mutations, as reported before, the IDH2 R172K was mutually exclusive with NPM1 and/or FLT3-ITD mutations. Overall, there was a trend for increased OS for patients with IDH2 R172K (26 vs. 15 months) as compared to those with R140Q. Considering only patients with a normal karyotype and no NPM1/FLT3-ITD mutation, these patients (n=27) had a highly significant better OS than patients with IDH2 R140Q (46.3 vs. 13.1 months, p=.012), supporting the findings published by Papaemmanuil et al. (NEJM 2016).
In IDH1-mutated patients, we observed statistically significant differences in baseline characteristics between the two most common mutation types, IDH1 R132C and R132H. Patients carrying the R132C mutation were older (62 vs. 55 years, p=.001), had lower WBC (3.6 vs. 21 Gpt/L, p≤.001) and were less likely to have a normal karyotype (43% vs. 66%, p=.002), NPM1 (23% vs. 66%, p=<.001), and FLT3-ITD mutations (8% vs. 27%, p<.001) than those with the R132H variant.
In univariate testing, the CR rate was also statistically significant lower in patients with IDH1 R132C (53% vs. 72%, p≤.001), with a median OS of 12.9 months compared to 17.4 months for patients with R132H variant (p=.08). In multivariate analysis including age, WBC, NPM1 and FLT3 status, and ELN risk, the CR rate was significantly lower in patients with the IDH1 R132C variant (p=.038).
The median IDH VAF was 38% (range, 0.1 - 58) with no difference according to the different types of mutation. Patients with a VAF > 30% had a significantly higher BM blast count (73% vs 40% for VAF≤5%) and WBC (21.2 Gpt/L vs. 3.7 Gpt/L) at baseline, but there was no clear impact on CR rate or OS found in multivariate analysis.
Conclusion
In this large cohort of AML patients with IDH1/2 mutations, we found significant and so far not reported differences for one of the two most prominent mutations types of IDH1. The R132C variant was associated with increased age, lower WBC, and lower NPM1 and/or FLT3 co-mutation rate. Further, these patients had lower CR rates and a trend for shorter OS. For IDH2 we were able to reproduce findings on co-mutations and showed a favorable outcome for intensively treated patients with a normal karyotype and no NPM1/FLT3-ITD mutation and the IDH2 R172K variant, providing additional evidence for classification as a separate AML entity.
Middeke:Roche: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Membership on an entity's Board of Directors or advisory committees. Rollig:Bayer: Research Funding; Janssen: Research Funding. Kramer:Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Bayer: Research Funding; Daiichi Sankyo: Consultancy. Scholl:Alexion: Other: Travel support; Abbivie: Other: Travel support; Novartis: Other: Travel support; Deutsche Krebshilfe: Research Funding; Carreras Foundation: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees; MDS: Other: Travel support; Jazz Pharma: Membership on an entity's Board of Directors or advisory committees. Hochhaus:Incyte: Research Funding; Pfizer: Research Funding; Takeda: Research Funding; Bristol-Myers Squibb: Research Funding; Novartis: Research Funding. Brümmendorf:Takeda: Consultancy; Pfizer: Consultancy, Research Funding; Janssen: Consultancy; Merck: Consultancy; Novartis: Consultancy, Research Funding. Burchert:Novartis: Research Funding; Pfizer: Honoraria; Bristol Myers Squibb: Honoraria, Research Funding; AOP Orphan: Honoraria, Research Funding; Bayer: Research Funding. Krause:Novartis: Research Funding. Hänel:Amgen: Honoraria; Novartis: Honoraria; Roche: Honoraria; Takeda: Honoraria. Platzbecker:Celgene: Research Funding. Mayer:Johnson & Johnson: Research Funding; Roche: Research Funding; Eisai: Research Funding; Affimed: Research Funding; Novartis: Research Funding. Serve:Bayer: Research Funding. Ehninger:Cellex Gesellschaft fuer Zellgewinnung mbH: Employment, Equity Ownership; Bayer: Research Funding; GEMoaB Monoclonals GmbH: Employment, Equity Ownership. Schetelig:Gilead: Consultancy, Honoraria, Research Funding; Abbvie: Honoraria; Janssen: Consultancy, Honoraria; Roche: Honoraria; Sanofi: Consultancy, Research Funding; Novartis: Consultancy, Honoraria, Research Funding. Thiede:AgenDix: Other: Ownership; Novartis: Honoraria, Research Funding. Stoelzel:Neovii: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal